Archive
The Next Big Health App Needs to Do More Than Just Track Our Numbers | Gadget Lab | Wired.com

This week we got a deep look at the rumored new health and fitness tracking application for Apple’s next iPhone, called Healthbook. Supposedly, Healthbook will not only track things like how much exercise and sleep you’re getting, but also your blood pressure, your blood sugar levels, and much more. All that collection will be great, but without a way to not just collate them, but make them meaningful, it runs the risk of becoming data clutter.
Parochial restrictions on telemedicine will become irrelevant when smartphone apps effectively aggregate healthcare data to help individuals become and stay healthier. It is only a matter of time when face to face interaction between healthcare providers and their patients become the exception rather than the rule. Physicians will be able to devote their time to sicker patients while still monitoring their healthier patients to keep them healthy.
See on www.wired.com
Doctors on Twitter: 2006 – 2014 Worldwide growth mapped #hcsm
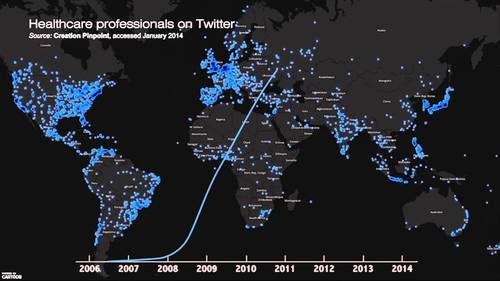
[Video maps growth in doctors, nurses and healthcare professionals using Twitter since its launch in 2006 to 2014.]
While Facebook lends itself better as a professional social media portal, it would be interesting to know the growth in patients’ following their physicians on Twitter (and other social media). If we can get past the hurdles of HIPAA restrictions and other legal silliness, social media could become the mechanism through which patients and their physicians effectively interact and improve their healthcare.
See on www.youtube.com
Steps 3, 4, 5, 6, and 7 in Doing a Healthcare Deal (Correctly)

Step 3 – Identify the governmental agencies that have authority over the deal
- Are there any notices or approvals required?
- What are the licensing requirements?
- Will a change in control occur?
- Is a new provider application/number needed?
- Is a CON needed? An inspection?
- What effects will the deal have on any accreditation needed by the parties?
- What is the timing of agency requirements vs. closing the deal?
Step 4 – Identify the third party payors that will be involved
- Are the services to be performed as a result of the deal reimbursed by Medicare?
- Medicaid?
- Other federal or state programs?
- Commercial payors?
- What credentialing/provider applications are needed?
- Do any payors have special requirements that must be satisfied before closing the deal?
Step 5 – Identify the due diligence requirements
Remember that a healthcare deal starts like any other deal, and the parties must do their basic due diligence about each other
- Entity organization and ownership
- Legal authority
- Financial statements, assets and liabilities, liens
- Contracts and commitments, leases
- Employees and benefit plans
- Taxes
- Insurance
- Litigation
Step 6 – Identify the healthcare due diligence requirements
- Licenses and requirements applying to transaction
- Equipment and inventories
- Cost reports, inspections, regulatory correspondence
- Quality of care, malpractice claims/insurance
- Patients records, EHR compatibility, billing software
- Managed care/provider agreements, liability, assignability
- Subcontractors/suppliers
- Stae law requirements
- Fair market value
- Commercial reasonablenessFair market value and Commercial Reasonableness — These are the critical underpinnings of every healthcare deal. What is being given, what is being received, and is it commercially reasonable?Get an opinion from a qualified healthcare valuation expert to support the FMV.
Step 7 – Document the Deal
- Documentation is a critical step in protecting the parties, achieving the goals of the deal, and meeting compliance requirements. Stark Exceptions and Anti-Kickback Safe Harbors impose specific requirements on deal documentation.
- Should the parties enter into a nonbinding letter of intent/memorandum of understanding?
- Pros – helps the parties determine whether there has been a meeting of the minds prior to devoting substantial time and expense and helps manage expectations and reduce surprises.
- Cons – can consume an inordinate amount of time prior to due diligence being completed and lock the parties into unrealistic positions.
 Next time — How to screw up the deal that everyone wants.
Next time — How to screw up the deal that everyone wants.
Justice Department Hits Physician Owned Distributorships (PODS)
Florida Healthcare Law Firm Blog
 For the first time, the Department of Justice (DOJ) has fired a shot at a
physician owned distributorship
(POD). In the case, the DOJ suit claims that the ownership interest of a neurosurgeon in a spinal surgery device distributorship has caused him to perform unnecessary surgeries.
For the first time, the Department of Justice (DOJ) has fired a shot at a
physician owned distributorship
(POD). In the case, the DOJ suit claims that the ownership interest of a neurosurgeon in a spinal surgery device distributorship has caused him to perform unnecessary surgeries.
PODs have been the source of considerable controversy for years. A couple years ago, they caught the attention of Congress. The Office of Inspector General of the Department of Health and Human Services (“OIG”) has even issued a Fraud Alert making clear their dislike of PODs and sending a clear shot across the bow of those who are in that industry. In 2006, the Office of the Inspector General of HHS and CMS expressed major concerns about PODs, and cited concerns about “improper inducements.” At that time, the OIG stopped short of prohibiting them, but called for heightened scrutiny. CMS itself has stated…
View original post 1,086 more words
Phoning It In – Florida’s Brand New Telemedicine Law
Florida Healthcare Law Firm Blog
 By:
Jackie Bain
By:
Jackie Bain
Until recently, the State of Florida has successfully avoided regulating telemedicine to account for advancements in technology. In 2003, the State issued standards for telemedicine prescribing practice for medical doctors and doctors of osteopathy, but has not formally revisited its position in light of increasingly common telemedicine practice in several states – until now.
Florida’s forestalling has officially come to an end. The State recently enacted new physician standards for telemedicine practice, and the State legislature is presently considering further regulation. These new standards do not impinge upon the prior standards for telemedicine prescribing practice, but are issued in conjunction to it.
View original post 304 more words
Steps 1 and 2 (of 7) in Doing a Healthcare Deal (Correctly)
Step 1 – Describe and Understand the Deal
- Why?
- What is it that is hoped to be accomplished?
- Why is that a good outcome?
- Does it make sense? I.e., is it commercially reasonable?
- Is the deal more than just about referrals and money?
- What happens if a regulator “follows the money”?
- How will the deal affect others – patients, employees, physicians, competitors, the community, etc.?
- What are the tax effects?
- Engage legal, accounting, valuation, and other professional consultants early in the process to review the proposed deal.
Step 2 – Identify the Parties to the Deal
- Who is involved (medical professionals, background)?
- Why are they involved?
- What do they bring to the deal?
- When did they get involved?
- Who got them involved?
- What does each party hope to achieve?
- Are the goals reasonable?
- Are the goals legal and ethical?
Dos and Donts of Deal Making in Healthcare
Last week, I presented at a webinar sponsored by the American Association of Orthopaedic Executives. The topic dealt was “2014 Healthcare Compliance.” You can access the entire PowerPoint presentation at SlideShare.
I spoke about the dos and don’ts of healthcare deal making. The focus was on deals with physicians, but the concepts are applicable to deals involving all types of healthcare providers. Below I summarize my Rules of Thumb for healthcare deals:
Rules of Thumb for Healthcare Deals
- RULE #1: Just because a proposed deal makes sense and would be appropriate in a business other than healthcare, doesn’t mean it’s legal. (Corollary — Just because everyone is doing it, doesn’t mean it’s legal.)
- RULE #2: Determining the legality of a healthcare deal can be complicated, time consuming, expensive, and inconclusive.
- RULE #3: The risks of doing an illegal healthcare deal far outweigh the benefits.
- RULE #4: Get professional help early in the deal.
In subsequent posts, I will discuss steps in the deal and ways to screw up the deal.
The Need for Physician Leadership Development
It is critical now that medical practices take the steps needed “to retain, develop, and align [its] medical staff to meet the challenges of a fast-changing and highly competitive healthcare landscape.” Good physician leaders can help achieve those goals. This is the message in a recent post from Physicians Practice, “Medical Practices Must Focus on Physician Leadership Development.”
Equally important, however, is the need for physician leaders to see and develop opportunities as a result of forces in the very fast moving healthcare environment outside of their own medical practices.
Questions, like the following, are constantly swirling around medical practices, and I fear they are as often ignored as they are avoided:
- Should we align with the hospital?
- Should we join a large physician group?
- Should we develop our own super group?
- Should we join the hospital sponsored clinically integrated network?
- Should we start our own network?
Hospitals and venture capitalists have the money, the time, and the leadership to develop and pursue healthcare business opportunities, and they are doing so. They are taking the lead in presenting answers to these questions. Physicians are at a disadvantage, because they rarely have the money or the time or, unfortunately, the leadership to be proactive in evaluating and accepting or rejecting opportunities as they present themselves.
If survival as independent practices is the goal, then in this highly competitive business environment, physician leadership has never been more important. This has been the message of many physician practice commentators, including Kevin Pho, M.D. on his blog, as well as physician leadership training programs like the one done at the University of Cincinnati.
No one is waiting for physicians to step. When they do, they can control their professional destiny. When they don’t or can’t, others will be in control.
Avoid Being the Ostrich
A recent post on the Deloitte Center for Health Solutions Blog, “Convergence in health care: The opportunity in uncertainty,” starts off with the following statement:
There is no question that significant change is occurring in the health care industry and nobody really knows exactly how all of this is going to play out over the next couple of years. In light of all of this uncertainty, one of two scenarios could have played out: players in the health care industry could have sat on the sidelines, waited it out to see what happens, and avoided the potential risk that comes with uncertainty. Instead, the alternative scenario is playing out with organizations across all parts of health care using change as an opportunity to make bold plays from a strategic perspective. Some of that is manifesting itself in consolidation within sectors, and some of that is manifesting itself in convergence across sectors.
I agree.
As I tell my healthcare clients, the roller coaster healthcare environment presents them with many alternative business opportunities. However, one alternative that must be avoided is doing nothing. Doing nothing is not the same as staying where you are. The status quo may be the right strategy for some. For others, it may be consolidation and convergence. But everyone needs to stay focused and be an active participant in his or her business future. Involvement is required to evaluate the different alternatives and make a good decision. Otherwise, opportunities will be lost and maybe lost forever.
Florida Cares About Healthcare … Not
I have been very remiss about posting for the last several weeks.
Being a Floridian is very depressing. Florida’s elected and administrative leaders have done everything they can to misinform Floridians about Obamacare, to keep the needy from accessing care, to prevent the uninsured from being able to purchase affordable health insurance, and to force healthcare providers to provide unreimbursed care.
Earlier today, Health News Florida reported on how politics over healthcare reform has become more important than either healthcare or meaningful reform.
- The New York Times reported on Tuesday that “Gov. Rick Scott and the Republican-dominated [Florida] Legislature have made it more difficult for Floridians to obtain the cheapest insurance rates under the exchange and to get help from specially trained outreach counselors.”
- The Miami Herald reported also on Tuesday that HHS Secretary Kathleen Sebelius, stated that Florida officials are “keeping information from people” in a political effort to foil the effort to enroll Floridians for health insurance.
- Florida AG Pam Bondi and CFO Jeff Atwater have also joined in the campaign of misinformation and deceit.
The list of wasted Florida tax dollars and loss of Federal funding in trying to impede Obamacare was reported by Health News Florida earlier this week. Florida’s list of shame includes the following:
- Leading the court challenge on the constitutionality of Obamacare in 2010 soon after it was signed into law. Attorney General Pam Bondi made it one of her high-profile issues, becoming a regular guest on Fox News to attack it.
- After the Supreme Court ruled the law was constitutional, the Florida Legislature told state agencies not to implement it because lawmakers felt sure the Republican party Presidential candidate, Mitt Romney, would win the election in 2012 and repeal the law.
- After Romney lost the election, governor and legislature pressured the agencies not to apply for grants related to the law; some agencies had to give back grants they had already been awarded.
- The Legislature this year voted against Florida having its own electronic marketplace for health-plan shopping, even though the state had already spent five years and several million dollars building an online shopping site, Florida Health Choices, that has yet to be used.
- After months of hearings and negotiations, the Florida Senate came up with a compromise plan on Medicaid expansion that would accomplish several things — reduce the number of uninsured Floridians by about 1 million by using federal funds, save millions of state dollars now being spent on the uninsured, and continue privatization of the Medicaid program, already well under way. But the House said no.
- The Legislature voted to strip the Insurance Commissioner’s authority to regulate health premiums for two years.
- Insurance Commissioner Kevin McCarty issued a report that predicted health premiums in Florida’s individual market would soar 30 to 40 percent, thereby producing scandalous headlines. Later, others would note that the figure failed to make adjustments for the tax credits most of those shopping in that market would qualify for. He also failed to mention that the sector he was describing accounts for only 5 percent of policies.
It’s all really quite pathetic and disgusting. It’s time to vote the bastards out.
